Interfejsy mózg-komputer (BCI, ang. Brain-Computer Interfaces) to urządzenia, które rejestrują sygnały aktywności mózgu, analizują je i ‘tłumaczą’ na polecenia przekazywane do urządzeń wyjściowych. W ten sposób systemy BCI są niezależne od tradycyjnych dróg komunikacji które ma do dyspozycji ludzki mózg (z wykorzystaniem nerwów i mięśni obwodowych). Ze względu na tę unikalną cechę urządzenia tego typu mogą w przyszłości umożliwić osobom niepełnosprawnym, w tym całkowicie sparaliżowanym, korzystanie z komputera i innego sprzętu technicznego na równi z innymi użytkownikami.

Research directions
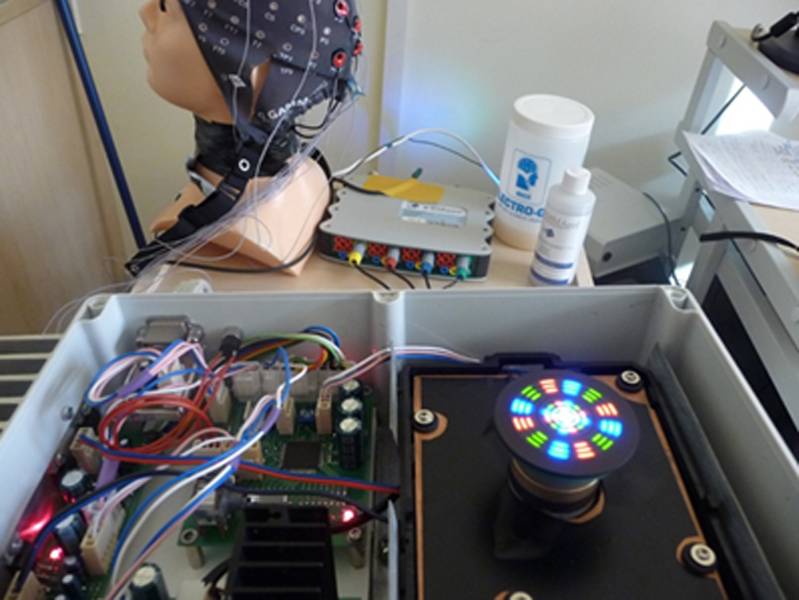
Studies on the development of the BCI devices have more than 30-years of history. The most widely represented group of devices are non-invasive BCI systems with electroencephalographic (EEG) brain activity monitoring. The most commonly used EEG-based BCI systems employ commonly known paradigms: an event-related synchronization of µ and β rhythms (ERD/ERS), event-related potentials (ERP) and steady-state visual evoked potentials (SSVEP). Different mental commands have diverse, perspective applications – from rehabilitation, through biofeedback techniques to human augmentation.
Nowadays much research activities concentrate on hybrid BCI systems (combining more than one BCI paradigm), multi-modal communication systems and signal analysis algorithms, especially spatial filtering and detection methods.

0
Achievements
Instead of using classical spectrum analysis method in order to extract steady-state visual evoked potentials (SSVEPs) from the recorded brain activity of the interface user we developed an alternative based on Canonical Correlation Analysis. This modification allows finding the best bipolar combination of measurement channels (one used as a signal channel, the other as a reference).
The proposed detection algorithm improves classification accuracy in the groups of subjects with the average and poor results (rated based on classical spectrum analysis method). In the group of users with the best results, there was no clear improvement of the SSVEP detection accuracy. At the same time average detection times were not significantly better, but the measured overall information transfer rates were in many cases higher for the proposed method, which is due to higher classification accuracy of this method. It should be noticed that only a short off-line calibration session was necessary to achieve such results.
0
Perspectives
Due to a high user SSVEP variation, BCI illiteracy phenomenon, and a low communication speed many BCI systems are still at the stage of laboratory demonstrations or small-scale clinical trials with promising results for patients with various neurological diseases. In our opinion, these limitations may be eliminated in the following years by improvement of portable EEG technologies (enabling reliable and effective use of an EEG recorder in home environments) as well as further development and optimization of BCI algorithms, spatial filtering and detection methods so that they can work reliably in uncontrolled environments.
0